

New Diagnostic Radiology Oral Exam
On this page
- First Edition of Candidate Guide Posted (July 23, 2026)
- ABR Trustee Explains How Oral Exams Allow Candidates To Share Their Knowledge (June 15, 2026)
- ABR Newsletter Features Helpful Articles About Oral Exams (June 10, 2026)
- ABR Executive Director Brent Wagner, MD, MBA, Appears on RSNA’s Podcast (May 15, 2026)
- Advisory Committee Members Talk About the New DR Oral Exam (May 6, 2026)
- DR Exam Changes: Timing Impacts for DR Residents (December 12, 2025)
- DR Oral Certifying Exam Sample Cases Available (January 20, 2025)
- DR Oral Exam Reenactment (November 27, 2024)
- New Exam Builds on Previous Model with Scoring Rubrics (November 4, 2024)
- Exam Development Update (May 9, 2024)
- Differences in Qualifying (Core) and Certifying Exams (May 3, 2024)
- First-year Resident Discusses the Exam (April 17, 2024)
- Oral Exam Update (November 14, 2023)
- Addressing Questions About the New Exam (June 28, 2023)
- Town Hall Recording Available (May 11, 2023)
- Transition to New DR Oral Exam (April 13, 2023)
- New DR Oral Exam FAQs
- Evaluating Potential Solutions (October 2022)
- Call for Stakeholder Comments (May 2022)
2026
July 23
First Edition of Candidate Guide Posted
One of several resources the ABR offers to help trainees along their path to board certification is a candidate exam guide. This handbook gives candidates vital information to prepare for using the remote exam software, including technical and location requirements, accommodations, and exam day logistics.
ABR staff and volunteers recently completed initial work on the Diagnostic Radiology Candidate Exam Guide and posted it on our website. The guide will be continually updated through the first administration in 2028. A separate candidate study guide will focus on exam content (coming soon).
If you have questions after reviewing the guide, please contact an ABR certification manager at information@theabr.org. More information about the DR Oral Exam can be found on our website.
June 15
ABR Trustee Explains How Oral Exams Allow Candidates To Share Their Knowledge
June 10
ABR Newsletter Features Helpful Articles About Oral Exams
The latest issue of The Beam, the ABR’s newsletter, includes two articles that should be of interest to diagnostic radiology candidates who will be taking the oral certifying exam.
The first addresses myths surrounding the exam, including the false notions that examiners are trying to “trick” candidates or that the ABR has a set range for a passing rate.
The other explains how exam scoring is determined. This method applies to all ABR oral exams, not just the DR version.
Please continue reading The Beam, our blog, and this page for news about the exam. You may also consider following us on our social outlets (Blue Sky, Facebook, Instagram, LinkedIn, Threads, and X) and subscribing to our YouTube page.
May 15
ABR Executive Director Brent Wagner, MD, MBA, Appears on RSNA’s Podcast
May 6
Advisory Committee Members Talk About the New DR Oral Exam
2025
December 12
DR Exam Changes: Timing Impacts for DR Residents
After months of soliciting feedback from stakeholders, the ABR is making changes to the timing of the Qualifying (Core) and Certifying exams for diagnostic radiology (DR) trainees.
The ABR hosted a webinar with program directors on November 10 to answer questions about implementation of exam timing. You can find the recording on our YouTube page.
DR Exam Timing
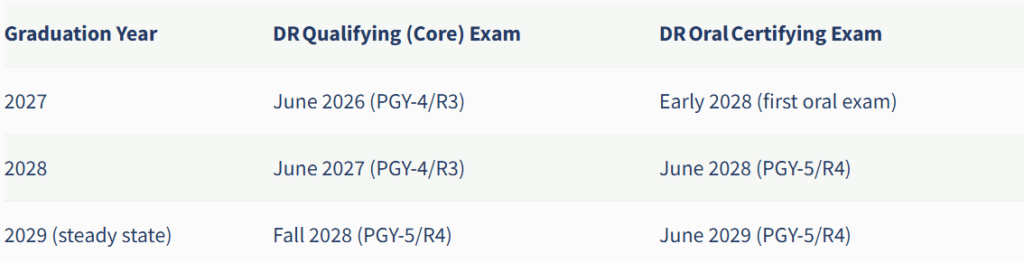
DR residents will see the timing of their exams change starting in 2028. In a steady state, DR residents will have their first opportunity to take the Qualifying (Core) Exam in the fall of their PGY-5/R4 year and their first opportunity to take the Oral Certifying Exam in June of their PGY-5/R4 year.
Details about the transition plan for DR residents graduating in 2027-2029:
If you have questions, please contact the ABR at information@theabr.org or 520-790-2900.
January 20
DR Oral Certifying Exam Sample Cases Available
Our diagnostic radiology Trustees have created a set of sample cases to give an idea of the types of topics and depth that will be evaluated on the exam. The sample text describes what a candidate should be able to identify and discuss regarding the images. The focus is on allowing candidates to demonstrate their skills in observation, synthesis, and management. The exam is still under development, and these are not actual cases that will be used. The intention is to provide a general idea of the content and format.
2024
November 27
DR Oral Exam Reenactment
ABR volunteers Desiree Morgan, MD, and Derek Sun, MD, run through a simulated DR oral exam. Dr. Morgan and ABR Associate Executive Director for Diagnostic Radiology Mimi Newell, MD, then take part in a mock panel discussion. We also have posted oral exam sample cases on our website.
November 4
New Exam Builds on Previous Model with Scoring Rubrics
The development of the new DR Oral Exam model benefited from iterative contributions of a wide range of external stakeholders, and the subsequent decision to return to an oral exam format was largely focused on a specific goal: to create an exam that assesses the higher order skills that are part of clinical practice (in contrast to knowledge assessable on a multiple-choice exam).1
In communications related to the change, the ABR compared the 2028 model with the legacy ABR oral exam that existed for decades through 2012. In conveying that the 2028 version will be different from the old DR oral exam, we have unintentionally created the impression for some faculty and candidates that we have not retained some of the attributes and principles of the legacy exam.
The previous and upcoming models both represent composite assessments based on cases presented by and discussed with several examiners during a series of 25-minute one-on-one sessions covering the different subspecialty content areas of radiology. Candidates analyze cases based on their observations of the imaging features and available history and summarize their findings in the form of a reasonable differential diagnosis before suggesting next steps (e.g., additional imaging, urgent referral for consideration of surgery, etc.). The analysis by the candidate resembles a succinct summary that might be part of a multidisciplinary conference, a concise but complete report, or a phone conversation with the treating physician. The examiner might ask clarifying questions or redirect the candidate to the major findings or alternative diagnostic possibilities. Each candidate is assessed by the specific group (panel) of examiners who discussed the cases with them. In the panel discussions, scores for individual sections may be raised if low performance in a particular subject area is considered an outlier.
The most obvious difference in the new exam is that it will be administered remotely using a one-on-one videoconference format. Less apparent to the candidate will be our efforts to mitigate subjectivity and bias in the exam. For example, cases will be given in the same order for each session, and each category will have an identical case set for a given oral exam date. As a result, all candidates examined on a Tuesday will see very similar content (although the number of cases might vary, depending on how quickly the examiner and the candidate can complete a case and move to the next).
Examiners in the old model used a general scoring grid that included three broad categories: observation (identifying the abnormality and pertinent negatives), synthesis (differential diagnosis, including the most likely diagnosis), and management (for example, additional imaging or urgent referral). The new model will build on these by defining specific elements (a rubric) to be used by all examiners as part of the electronic score sheet for each case.
For example, a conventional set of abdominal radiographs in a young adult with vomiting might demonstrate distended loops of gas-filled small bowel. A pertinent negative would be the absence of free air. A second finding would be a subtle lucency overlying the right inguinal region. Additional testing would be a CT scan with intravenous contrast. The major CT finding would be a right inguinal hernia containing thickened ileum with diminished enhancement. The overall management (urgent surgical consultation) would be based on a presumptive diagnosis of ischemic bowel within an incarcerated inguinal hernia. More detailed examples of performance rubrics are being prepared for the seven content areas by the ABR’s subject matter experts in diagnostic radiology and are scheduled to be posted on the ABR’s website by November 25.
The major goal of the new exam model is to assess the knowledge and skill of diagnostic radiologists. To that end, residents should prepare for the exam in a way that allows them to identify and appropriately communicate the presence and nature of imaging findings, the potential significance of those findings, and reasonable recommendations for next steps. The use of defined rubrics for each case will enhance standardization of objective scoring of the discussions.
- Larson DB, Flemming DJ, Barr RM, Canon CL, Morgan DE. Redesign of the American Board of Radiology Diagnostic Radiology Certifying Examination. Am J Roentgenology 2023;221(5). https://www.ajronline.org/doi/10.2214/AJR.23.29585
May 9
Exam Development Update
May 3
Differences in Qualifying (Core) and Certifying Exams
The Diagnostic Radiology Qualifying (Core) Exam will continue to assess the full scope of the discipline with an organ system approach and includes a robust examination of DR physics, radioisotope safety, and noninterpretive skills (NIS).
The new Diagnostic Radiology Oral Certifying Exam will include representative cases across seven categories* and will include basic diagnostic radiology procedures where appropriate. The candidate should anticipate discussing practical and clinically relevant physics and safety principles in the context of cases. The case discussions will assess the clinical, observation, communication, and professionalism skills required of an independently practicing diagnostic radiologist.
*Categories: Abdominal, Breast, Cardiothoracic, Musculoskeletal, Neuroradiology, Nuclear, and Pediatric.
April 17
First-year Resident Discusses the Exam
2023
November 14
Oral Exam Update
June 28
Addressing Questions About the New Exam
May 11
Town Hall Recording Available
April 13
Transition to New DR Oral Exam
Beginning in calendar year 2028 and first applying to DR residents completing training in June 2027 (entering their R1 year in July 2023), the certifying exam for DR will be the new DR Oral Exam. From that point on, a candidate’s first opportunity to take the new DR Oral Exam will be the calendar year following completion of their DR residency. All DR candidates taking the DR Certifying Exam after 2027 will be required to take the new DR Oral Exam regardless of when they completed residency training. We anticipate having two exam administrations per year.
The DR Qualifying (Core) Exam’s content, format, and timing will remain unchanged.
As part of continuing efforts to improve testing, particularly in light of technologic advancements implemented during the pandemic, the new DR Oral Exam will be an online exam taken in a location of the candidate’s choosing.
The new DR Oral Exam will include select critical findings as well as common and important diagnoses routinely encountered in general DR practice, focusing on examples that optimally assess observation skills, communication, judgment, and reasoning (application of knowledge learned during residency).
It is not meant to represent a comprehensive review of clinical content. The oral exam aims to assess higher-level skills that are needed to be an effective diagnostic radiologist and are valued by referring physicians and patients.
To mitigate subjectivity and potential bias inherent in an oral exam, examiners will use a standard set of cases, and detailed rubrics will be used to score each candidate. This is an improvement over the prior oral exam model and is facilitated by current technology, including software developed specifically for this purpose by the ABR and currently used for oral exams in the three other disciplines (interventional radiology, radiation oncology, and medical physics). As in the past, examiner panels will meet after each session to discuss candidate results to ensure fairness and consistency. A conditioned exam result will be possible. The panels will be balanced for geography, gender, and new vs experienced examiners.
For more detailed information about the new DR Oral Exam, please see our frequently asked questions (FAQs). We will be sharing additional information and guidance for exam preparation over the coming years.
DR Oral Exam FAQs
Format
In what ways will the new DR Oral Exam be the same as the previous DR Oral Exam (2013 and earlier)?
The candidate will meet with one examiner at a time. Each session will use a standard set of cases for each exam category. The examiner will display case materials to the candidate and ask questions related to the content being displayed. The breadth of content will be similar to the previous oral exam.
How will this be different from the previous DR Oral Exam?
The new DR Oral Exam will be delivered remotely via a platform that allows real-time case presentation and discussion between the examiner and candidate.
Content
What clinical categories will be included in the new DR Oral Exam?
There will be seven individual exam sessions. The clinical categories are breast, cardiothoracic, abdominal (includes gastrointestinal, genitourinary, and ultrasound), musculoskeletal, nuclear radiology, pediatrics, and neuroradiology. Diagnostic radiology procedures, professionalism, and safety will be incorporated into the clinical categories as appropriate.
How advanced will the cases be?
The content will include critical findings as well as common and important diagnoses routinely encountered in general practice.
What content should be expected in interventional radiology?
Because interventional radiology/diagnostic radiology (IR/DR) has a unique primary certificate and residency training pathway, performance of advanced interventional procedures (e.g., embolization, stent placement, thrombectomy, vertebroplasty, etc.) will not be covered in the new DR Oral Exam. However, knowledge of anticipated imaging findings and complications after interventional procedures will be part of the new DR Oral Exam.
In addition, DR procedures (e.g., image-guided biopsy, abscess drainages, arthrocentesis, lumbar puncture, etc.) will be covered, including indications, contraindications, techniques, anatomic considerations, and complications.
Will there be physics content?
Selected physics concepts that are directly related to safety will be incorporated as appropriate.
Will there be normals?
Examiners will not show normal cases as primary questions. In theory, normal images could be shown as a subsequent part of the case (e.g., if a follow-up study is indicated). Normal variants might be shown as primary questions, to assess the candidate’s ability to differentiate them from pathologic processes.
How will ultrasound be represented on the exam?
Ultrasound will be examined in a way that feels “organic,” in that it will appear during exam sessions where it generally would in routine practice. Specialized ultrasound studies, including thyroid, fetal, and vascular, will be examined in the abdomen section.
Will procedures and noninterpretive skills be tested?
Yes, both areas will be incorporated into exam content. Basic diagnostic procedures might be examined as part of a broader case discussion. Noninterpretive skills content will concentrate on areas of safety and professionalism, often as part of another case. Basic radiation safety and dose reduction principles might also be a subject of discussion. The examined content in both areas will be material that practicing radiologists might encounter on any given day.
Will I be expected to figure out what sequence is being shown on MRI cases?
No. MRI studies will be labeled for sequence type (e.g., T1 with contrast, T2, DWI). The ABR Image Quality Committee and the Board of Trustees think that having candidates spend exam time identifying sequences would not add value to the exam experience. The rare exception might be a case where recognizing the specific sequence is the concept being tested (e.g., in-phase vs out-of-phase imaging in the abdomen, or “silicone-only” image on a breast implant study).
How will the ABR inform residency programs what will be covered so they can help prepare their residents?
The ABR will communicate with program directors regularly to ensure a smooth transition. In addition, exam preparation resources will be posted on the ABR website as exam development processes proceed.
Will a study guide be provided?
Yes. A study guide will be posted on the ABR website well in advance of the first new DR Oral Exam administration.
Timing
What are the expected times for the exam for the first year and subsequent years?
In 2028, we will have winter, June, and fall administrations. The winter and June administrations will be available only for specific groups (please click here for details). Starting in 2029, there will be two annual administrations: one in June and one in the fall. Each administration will likely consist of four or more one-day exam periods (each candidate will need to set aside only one day to take their exam). Exam dates will be posted on the ABR website approximately 18 months before the first exam.
Will this have any impact on the DR Qualifying (Core) Exam?
There will be no changes to the Qualifying (Core) Exam content. Residents graduating in 2029 and later will be eligible to take the Qualifying (Core) Exam in the fall of their R4 year rather than in June of their R3 year.
Process
How many times can I take the new DR Oral Exam?
Candidates are eligible to take the exam through the end of their board eligibility, which extends six full calendar years after the completion of residency training. From 2029 onward, we will have two administrations of the DR Oral Exam each year. Please click here for more details about exam timing.
What if the candidate has a conflict of interest with the examiner?
Candidates and examiners are provided the opportunity to identify and report conflicts on exam day prior to the first session. Conflicts are resolved before the start of the exam. If neither party identifies a conflict before the exam but realizes that one exists as they greet one another, the exam period will be rescheduled with a different examiner.
What if the candidate has a complaint about an examiner?
Candidates should contact the ABR immediately following the completion of their exam if they have concerns about their exam administration.
What are the computer requirements, camera requirements, bandwidth requirements, etc. for the exam?
The technical requirements for candidates are not extensive. Details can be found in the Diagnostic Radiology Oral Exam Guide (coming soon).
What are my options for selecting a remote exam location?
This will be an online exam taken in a location of the candidate’s choosing. Details can be found in the Diagnostic Radiology Oral Exam Guide (coming soon).
Will the candidate be able to adjust (magnification, contrast, etc.) the images in real time?
Yes. The exam software allows a candidate to modify an exam image in real time during the exam. By default, candidates have this capability at the start of every case.
Will the exam have scrollable stacks?
Yes. There will be scrolling stacks and other types of multimedia images.
What happens if technical issues interfere with the exam?
The schedule allows additional time to complete periods that were unfinished due to technical issues on the part of the candidate or examiner. ABR staff do everything possible to ensure that each candidate can complete the exam on the scheduled date. More than 99% of candidates in ABR oral exams in medical physics, interventional radiology, and radiation oncology have completed their exam on the scheduled day.
Before every remote exam, candidates can perform a technical check to test their computer system with the same software that is used in the exam. Candidates are strongly encouraged to take advantage of this opportunity, which allows for potential issues to be identified and addressed well ahead of exam day.
Will the criteria for who can sit for the new DR Oral Exam stay the same or change?
Eligibility criteria will not change. Candidates must successfully complete or be on track to complete their residency training, pass the Qualifying (Core) Exam, and pay applicable exam fees.
What is the cost for the exam?
The ABR makes significant efforts to control costs, with fiscal stewardship being a prime priority of the ABR Board of Governors. Exam fees are not expected to increase because of the return to the DR Oral Exam. The exam fees are available here.
Will my exam be similar in scope and depth to other candidates’ exams?
To facilitate every candidate’s opportunity to showcase their knowledge and skill, we are taking the following steps to optimize the standardization and fairness of the oral exam experience:
- We will provide standardized examiner training. Such training is already operationalized for the interventional radiology, medical physics, and radiation oncology oral exams and is continuously evaluated and improved.
- New examiners will be coached, mentored, and monitored.
- Case sets are determined in advance by a committee of subject matter experts (practicing radiologists) and will not vary from one candidate to the next on a specific exam day.
How will the exam be tested before the first administration to make sure it works well?
We anticipate employing our existing oral exam software, which is in use for other ABR disciplines and has been thoroughly tested. We do not expect new features will be needed for this exam.
When will the ABR begin recruiting examiners for the new DR Oral Exam?
Volunteer applications for DR oral examiners (and other volunteers) are being accepted now. Visit the Volunteer page for more information.
Scoring
What can you share about the evaluation and scoring process?
We will share information about the evaluation and scoring process at least one year prior to the first exam administration.
How will conditioning work?
We anticipate that candidates failing one or two clinical categories will receive an exam result of “conditional pass.” Candidates with a conditional pass exam result are required to repeat only the clinical categories they failed during the previous administration.
Will there be examiner panels that can “raise” a low score if the candidate does well in all other clinical categories?
Yes. This has been a long-standing part of the oral exam process. Examiners review the performance of each candidate at the end of each day to confirm the final exam result. All examiners must agree on the overall result for each candidate.
What efforts will be made to mitigate bias and subjectivity in the assessment of the candidates?
For each session and category, the examiner will use a standard set of cases for all candidates. Detailed rubrics will be used to score each candidate. This is an improvement over the previous oral exam model and is facilitated by current technology, including software developed specifically for this purpose by the ABR.
In category meetings before each exam session, examiners will preview that day’s case set to help level-set expectations for what constitutes a passing score.
Panel meetings at the end of each exam session will allow examiners to discuss the performance of candidates holistically to ensure fairness and consistency. The panels will be balanced for geography, gender, and new vs. experienced examiners.
Specific Use Cases
What is the impact on an Early Specialization in Interventional Radiology (ESIR) resident?
This change will not impact ESIR residents in DR residency programs.
What is the impact on a DR resident who then matches into an Independent IR residency?
A DR resident matching into an Independent IR residency who opts to take the DR Certifying Exam after 2027 will take the new DR Oral Exam.
What if I have failed or not taken the computer-based DR Certifying Exam by 2028? What exam will I take?
Beginning in 2028, all diagnostic radiology candidates will be required to take and pass the new DR Oral Exam to earn certification, regardless of when they completed residency training. We will provide two computer-based DR Certifying Exam administrations in 2027 to help with the transition.
What if I can’t take the new exam during the time it is offered?
We will have two administrations each year to allow flexibility.
What happens if I don’t pass before my board eligibility expires?
This policy is unchanged. Candidates failing to successfully complete the initial certification process within the board eligibility period are no longer considered by the ABR to be board eligible and are no longer permitted to designate themselves as such for communications or credentialing purposes. Candidates wishing to regain board eligible status must complete an additional year of training.
Are exam accommodations available under the Americans with Disabilities Act (ADA)?
Yes. The ABR offers ADA and lactating and expectant parent exam accommodations for all exams.
How will this affect the implementation of “mini fellowships” in the R4 year?
Training during the R4 year is determined by the residency program director and continues to be handled at their discretion.
2022
October
Evaluating Potential Solutions
In October 2022, a project planning group comprising members of the ABR Board began meeting weekly to evaluate potential solutions and to develop an exam proposal based on information learned during our call for stakeholder comments in May 2022. The planning group met regularly with a larger working group of Diagnostic Radiology Trustees and was supported by ABR staff and Jennings Healthcare Marketing.
Key stakeholder organizations representing the interests of residents, program directors, department chairs, private practice, and community radiology groups were contacted and asked to provide representatives who could participate in longitudinal feedback facilitated by Jennings. These representatives formed a single stakeholder group that convened on multiple occasions in November 2022 to discuss options for exam content, timing, and structure. Relying on this valuable input, the project planning group continued to meet through the end of 2022 and early 2023 to develop and refine options. The process culminated in a proposal for exam changes including a new oral certifying exam that was provisionally approved by the ABR Board of Governors at the February 2023 board meeting.
May
Call for Stakeholder Comments
In May 2022, the American Board of Radiology (ABR) began seeking stakeholder input and insights into the Diagnostic Radiology (DR) Initial Certification (IC) process. This review included both the Qualifying (Core) and Certifying Exams.
The comprehensive stakeholder input process was facilitated by our third-party partner, Jennings Healthcare Marketing. The process focused on gathering feedback and perspectives through multiple channels as the precursor to considering possible process modifications. Stakeholder input included three primary sources:
Targeted Stakeholder Organization Input. Given the large number of affiliated organizations in radiology, we focused on several key groups representing residents, program directors, department chairs, private practice and community radiology perspectives. Jennings helped facilitate multiple structured feedback sessions with these organizations’ executive leadership. In addition, the targeted organizations were encouraged to seek input from their constituency. Organizations were asked to submit a written synopsis of their feedback to the ABR as part of the process.
Other Stakeholder Organization Input. Recognizing the value of input from as many perspectives as possible, we also invited any interested organization to submit a written synopsis of their feedback to the ABR. We encouraged organizations to seek input from their constituency in their written comments. Recommended discussion points were provided for interested organizations.
Individual Stakeholder Input. We also provided the opportunity for individual input and feedback through the publicly available Diagnostic Radiology Initial Certification Feedback Survey, which was distributed through the ABR website, The Beam e-newsletter, and social media. The survey was available May 25-August 31, 2022.
We appreciate the engagement and thoughtful discussions we had with so many people during this time of focused stakeholder input, including the response to the individual stakeholder input survey.
Stakeholder Input Summary
Overview:
Most stakeholders share the viewpoint that the current DR IC process does not accurately measure what radiologists do. Stakeholders reported that:
- The current DR IC process needs improvement.
- Multiple-choice questions (MCQs) do not optimally assess the detection, interpretation, and communication skills of trainees.
- MCQs can adequately (though not optimally) assess knowledge; many reported that MCQs alone are not a sufficient measurement of knowledge, particularly in the DR Certifying Exam.
- The DR Certifying Exam occurs too long after graduation from residency.
What has been going well:
- Stakeholders noted the value of offering remote exams and recommended continuing this moving forward.
- Stakeholders praised the ABR’s increased transparency and solicitation of stakeholder input.
- Stakeholders believe image-rich exams are beneficial since they get closer to testing what they are intending to test.
- Stakeholders noted that test questions are vetted, though some reported that a few seem antiquated.
What has not been going well:
- Some stakeholders reported that the exam is moving away from testing general knowledge toward testing more specialized knowledge, which is in line with the direction the profession is moving.
- Some stakeholders noted that this transition is biased in favor of larger programs.
- Others noted that this move toward specialization is less useful for smaller or more rural practices, where it is more helpful to have broad knowledge across the multiple subspeciality areas that constitute the broad domain of diagnostic radiology.
- Many stakeholders reported that the certification process is a good measure of the requisite knowledge required to be a competent practicing radiologist, but it is a poor measure of a radiologist’s clinical competence as it pertains to interpretation skills, communication skills, and professionalism.
- Stakeholders reported that preparation for a multiple-choice exam leads to trainees answering as many test questions as possible in lieu of taking cases as a study and learning mechanism, which results in fragmented learning, limited critical-thinking, and practice deficits.
For more information, please contact us at information@theabr.org or 520-790-2900.




